Professor of Neurology; Vice Chair of Research, Department of Neurology, Associate Director, University of Cincinnati Neuroscience Research
University of Cincinnati
Our research
Our research team has made major advances in understanding the causes of brain hemorrhage or intracerebral hemorrhage (ICH). In 2002, our investigators found that risk factors for brain hemorrhage can vary based on location within the brain.1 There are two major causes of spontaneous brain hemorrhage, hypertension and cerebral amyloid angiopathy or CAA. Our research found that risk factors for lobar hemorrhage were more often related to CAA while for other regions of the brain, they were more likely related to hypertension. (Genetic and Environmental Risk Factors for Hemorrhagic Stroke Study (I and II)
In 2006, we found that brain hemorrhage related to the increasing use of blood thinners to prevent stroke, has made this type of hemorrhage as common as aneurysm rupture hemorrhage also called subarachnoid hemorrhage.2
In 2008 we were funded to perform a large study screening the entire genome to identify novel risk factors for brain hemorrhage in 2014, our study group found the first major genetic risk factor for non-lobar ICH in the Chromosome 1q22.3 This region and finding was later replicated both in brain hemorrhage, white matter disease and all stroke demonstrating that it is a major risk factor for the brain’s small vessels.4,5 (Genetic and Environmental Risk Factors for Hemorrhagic Stroke Study (III)).
In 2010, our study group was funded to recruit 1000 non Hispanic white, 1000 non-Hispanic black and 1000 Hispanic brain hemorrhage patients and 3000 controls from across 41 centers in the United States. This large study was focused on having equal power in disproportionately affected minority populations and has led to over 25 publications along with a recent publication in JAMA-Open Access that demonstrates both the similarities and differences in risk factors for brain hemorrhage by race/ethnicity and location in the brain. (Ethnic/Racial Variations of Intracerebral Hemorrhage (ERICH)) Study.
In 2016, we sought to learn more about the genetic association identified in 2014 and were funded to recruit a new cohort of 1000 cases of brain hemorrhage that would include special blood sampling to evaluate for how genes are expressed in the blood which can compare to the genetic variation that was originally identified. That research is nearing completion and if positive, we may be able to more clearly understand how the genetic association identified leads to a higher risk of brain hemorrhage which could lead to new treatments to prevent this deadly disease. (Genetic and Environmental Risk Factors for Hemorrhagic Stroke Study (IV))
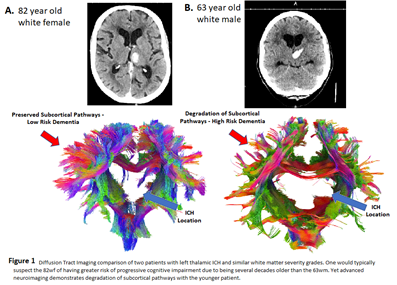
In 2017, we received funding for the Recovery and Outcomes from StrokE or ROSE study to include a special MRI or brain imaging technique that would allow us to see the brain’s tracts. These tracts or pathways may be stretched or destroyed by the brain hemorrhage and is a new way of being able to see the injuries that occurring.
In 2020, we received funding for the ROSE-Longitudinal Assessment With Neuroimaging study. This study is focused on the very high rate of patient’s developing dementia, a progressive deterioration of cognition or thinking and memory after an ICH. We had noticed this very high rate of progressive deterioration and combining with the imaging from the ROSE study and the gene expression changes, we may be able to determine if specific inflammation is leading to this progressive decline. If successful, we may have new targets that we can apply treatment that may prevent this progressive decline. We are studying the ability to ‘subtract’ one scan’s tractography from another scan gives us the ability to determine if progressive deterioration of those tracts are occurring.
References
Woo D, Sauerbeck LR, Kissela BM, Khoury JC, Szaflarski JP, Gebel J, et al. Genetic and environmental risk factors for intracerebral hemorrhage: Preliminary results of a population-based study. Stroke. 2002;33:1190-1195
Flaherty ML, Haverbusch M, Sekar P, Kissela BM, Kleindorfer D, Moomaw CJ, et al. Location and outcome of anticoagulant-associated intracerebral hemorrhage. Neurocrit Care. 2006;5:197-201
Woo D, Falcone GJ, Devan WJ, Brown WM, Biffi A, Howard TD, et al. Meta-analysis of genome-wide association studies identifies 1q22 as a susceptibility locus for intracerebral hemorrhage. Am J Hum Genet. 2014;94:511-521
Malik R, Chauhan G, Traylor M, Sargurupremraj M, Okada Y, Mishra A, et al. Multiancestry genome-wide association study of 520,000 subjects identifies 32 loci associated with stroke and stroke subtypes. Nat Genet. 2018;50:524-537
Neurology Working Group of the Cohorts for H, Aging Research in Genomic Epidemiology Consortium tSGN, the International Stroke Genetics C. Identification of additional risk loci for stroke and small vessel disease: A meta-analysis of genome-wide association studies. Lancet Neurol. 2016;15:695-707